

D&E ABORTION
Second Trimester
A dilation (dilatation) and evacuation abortion, D&E, is a surgical abortion procedure during which an abortionist first dilates the woman’s cervix and then uses instruments to dismember and extract the baby from the uterus. The D&E abortion procedure is usually performed between thirteen and twenty-four weeks LMP (that is thirteen to twenty-four weeks after the first day of the woman’s last menstrual period).
How is a d&e abortion performed?
To prepare for a D&E abortion, the abortionist uses laminaria, a form of sterilized seaweed, to open the woman’s cervix 24 to 48 hours before the procedure. The laminaria soaks up liquid from the woman’s body and expands, widening (i.e., dilating) the cervix.
When the woman returns to the abortion clinic, the abortionist may administer anesthesia and further open the cervix using metal dilators and a speculum. The abortionist inserts a large suction catheter into the uterus and turns it on, emptying the amniotic fluid.
After the amniotic fluid is removed, the abortionist uses a sopher clamp — a grasping instrument with rows of sharp “teeth” — to grasp and pull the baby’s arms and legs, tearing the limbs from the child’s body. The abortionist continues to grasp intestines, spine, heart, lungs, and any other limbs or body parts. The most difficult part of the procedure is usually finding, grasping and crushing the baby’s head. After removing pieces of the child’s skull, the abortionist uses a curette to scrape the uterus and remove the placenta and any remaining parts of the baby.
The abortionist then collects all of the baby’s parts and reassembles them to make sure there are two arms, two legs, and that all of the pieces have been removed.
what if a woman changes her mind after laminaria insertion?
If a woman has been dilated with laminaria, but not yet undergone the surgical abortion, she can still change her mind. Depending on how much her cervix has dilated, there is a potential risk of miscarriage as dilation continues because her body may begin contractions and labor. A woman who changes her mind should immediately contact a medical professional to ensure the laminaria is properly removed.1
-
Kaufman, K. The Abortion Resource Handbook.” New York: Fireside, 1997, 32, 153. <https://books.google.com/books?id=F7q3TB6_koYC&pg=PR18&dq=the+abortion+resource+handbook&hl=en&sa=X&ved=0ahUKEwjBpZvBxNrJAhUO42MKHchnCA4Q6AEIJjAA#v=onepage&q=the%20abortion%20resource%20handbook&f=false>.
Get Help
what are the short-term and long-term risks and adverse effects of medical abortion?
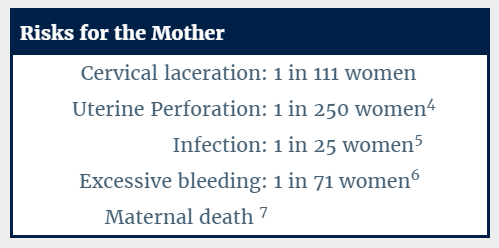
For the woman, this procedure carries a significant immediate risk of major complications. Since the baby is removed in pieces, sharp pieces of broken fetal bones can puncture the woman’s uterus or cause a large tear (laceration). This perforation or laceration of the uterus or cervix, can also possibly damage the bowel, bladder, the rectum and other maternal organs.
In addition to perforation and damage to internal organs, a second trimester abortion has a greatly increased risk of excessive bleeding and hemorrhaging. This is because the placenta is tightly adherent to the lining of the womb at this stage in pregnancy, and removing it often requires considerable scraping. The risk of excessive bleeding as a result of the abortion increases as the baby develops. The woman may also experience extreme blood loss if her uterus or cervix is injured, if the uterus does not contract properly after the procedure, or if she has an incomplete abortion. She also runs a higher risk of cervical damage, uterine perforation and scarred tissue, which may result in future pregnancy complications, such as miscarriage and preterm birth.1 Uterine rupture can even lead to maternal death.
Long-term damage from second trimester abortion is more frequent than for abortions in the first trimester. Because the cervix has to be so widely dilated to extract the larger child, the risk of cervical damage is much greater, increasing the risk that a woman will be unable to carry a future pregnancy to term. The CDC also estimates that the risk of death increases by 38% for each additional week of gestation.2
There are studies that indicate the risk of depression, anxiety, and suicide is greater for a woman who aborts an unwanted pregnancy than it is for a woman who carries an unwanted pregnancy to term.3
-
Lohr, Patricia A. “Surgical Abortion in Second Trimester”, Reproductive Health Matters, May 2008, 156. <www.ncbi.nlm.nih.gov/pubmed/18772096>.
-
Bartlett, Linda A., et al. “Risk Factors for Legal Induced Abortion–Related Mortality in the United States.” Obstetrics & Gynecology, Vol. 103, No. 4, April 2004, pp. 729-737. <http://www.ncbi.nlm.nih.gov/pubmed/15051566>.
-
Fergusson, David M with Joseph M. Boden and L. John Harwood. “Does abortion reduce the mental health risks of unwanted or unintended pregnancy? A re-appraisal of the evidence.” Australian & New Zealand Journal of Psychiatry, Sept. 2013, Vol. 47, No. 9, pp. 819-827. <http://www.ncbi.nlm.nih.gov/pubmed/23553240>.
-
Fox, Michelle C. and Jennifer L. Hayes. “Cervical Dilation in Second-Trimester Abortion.” Clinical Obstetrics and Gynecology. Vol. 52, Issue 2, June 2009, pp. 172-8 <http://journals.lww.com/clinicalobgyn/Abstract/2009/06000/Cervical_Dilation_in_Second_Trimester_Abortion.8.aspx>.
-
Cates, Willard Jr. and David A. Grimes. “Deaths from Second Trimester Abortion by Dilatation and Evacuation: Causes, Prevention, Facilities.” Obstetrics & Gynecology, Vol. 58, Issue 4, October, 1981. <http://www.ncbi.nlm.nih.gov/pubmed/7279335>.
-
Peterson, W.F., et al. “Second-Trimester Abortion by Dilatation and Evacuation: An Analysis of 11,747 Cases.” Volume 2, No. 2, Aug 1983. <https://venus.ipas.org/library/fulltext/PetersonOG1983.pdf>.
-
“Risk Factors for Legal Induced Abortion-Related Mortality in the United States.” American College of Obstetrics and Gynecology, Vol 103, No. 4, April 2004.
Are late-term abortions legal in the united states?
While some states have enacted prohibitions on abortion — including restricting the procedure after a certain point in pregnancy — other states permit abortions without exception.
how developed is the child at this point in pregnancy?
Week 13
At week thirteen LMP, the preborn baby’s fingerprints are visible, and the child’s organs are visible through his or her thin skin. The baby is roughly three inches long during this stage of pregnancy. Source: Baby Center.

Week 16
At week sixteen LMP, the child’s toenails begin to form, and his or her face and limbs are much more developed. The baby’s heart is pumping roughly 25 quarts of blood every day, and will continue as the child develops in the womb. Many mothers feel the baby move by this point in the pregnancy. Source: Baby Center.

Week 20
At twenty weeks LMP, the child’s nervous system is developed enough to feel pain. Research by the University of Toronto shows that babies at this stage can feel pain in the womb — even with greater intensity than adults. Almost all mothers feel the baby move by this point in pregnancy. Source: Baby Center.

Week 24
At twenty-four weeks LMP, the baby is roughly a foot long, and his or her brain is developing rapidly. The child’s lungs are also developing into their branch-like structure. At this age, almost all babies can survive outside the mother if given proper support. Source: Baby Center.

Please note: This website has been researched and reviewed by physicians for medical accuracy; however, it is not intended to constitute medical advice or replace the individualized counsel of a doctor.
ASPIRATION ABORTION
First Trimester Suction D&C
A suction, or aspiration, D&C abortion is a procedure in which a suction catheter is inserted into the mother’s uterus to extract the preborn baby. Tools are then used to scrape the lining of the uterus to remove any remaining parts. This procedure is performed during the first trimester, typically during five and thirteen weeks LMP (that is five to thirteen weeks after the first day of the woman’s last menstrual period).
How is an aspiration (suction) abortion performed?
A suction, or aspiration, D&C abortion is performed in-clinic. Prior to the abortion, the woman should receive an exam that includes an ultrasound in order to confirm that she is pregnant and diagnose any complicating factors, such as a tubal, or ectopic, pregnancy. An abortionist uses metal rods or medication to dilate the woman’s cervix and gain access to the uterus, where the baby resides. The abortionist then inserts a suction catheter to vacuum the child from the womb. The suction machine has a force approximately 10 to 20 times the force of a household vacuum cleaner. The procedure is completed as the abortionist uses a sharp metal device called a curette to empty the remains of the child from the mother’s uterus.1
A follow up exam and ultrasound can be performed to help minimize the risk of incomplete abortion.2
-
World Health Organization, “Safe Abortion: Technical and Policy Guidance for Health Systems.” 2nd Edition, 2012. <http://apps.who.int/iris/bitstream/10665/70914/1/9789241548434_eng.pdf>.
-
Debby, A, et. al. “Transvaginal ultrasound after first-trimester uterine evacuation reduces the incidence of retained products of conception.” Ultrasound in Obstetrics & Gynecology, Vol. 27, Issue 1, January 2006, pp. 61-64. <http://onlinelibrary.wiley.com/doi/10.1002/uog.2654/full>.
What are the short-term and long-term risks and adverse effects of an aspiration (suction) D&C abortion?
Injury to the uterus or cervix, potentially damaging intestines, bladder, and nearby blood vessels, may occur.1 Other consequences include hemorrhage, infection, and in some cases, even death of the mother.2
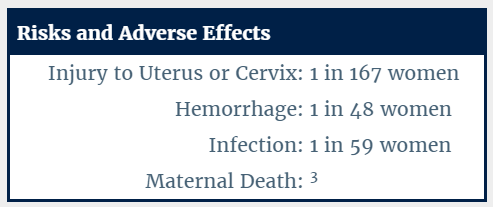
An “incomplete abortion” occurs when parts of the aborted baby are left in the uterus following the abortion (approximately 1 out of 63 Suction D&C abortions is incomplete).4
Extreme pain, nausea, excessive bleeding, and even death may result from an incomplete D&C abortion. A woman may need surgery to remove the fetal body parts as well as blood transfusions and antibiotics.
Long-term, D&C abortions have caused complications in future pregnancies. One such complication that it can make it difficult to carry a future pregnancy to term. D&C abortions have been known to cause damage to the uterus or cervix, which can result in very premature births with the next pregnancies.5 The subsequent scarring to the uterus6 may increase the risk of uterine rupture during future pregnancy, which may result in death of the baby and even the mother.7,8. In addition to an increased risk of preterm birth, damage to the lining of the uterus can also cause additional problems for the woman during future deliveries, including significantly higher risk of hemorrhaging.9
There are studies that indicate the risk of depression, anxiety, and suicide is greater for a woman who aborts an unwanted pregnancy than it is for a woman who carries an unwanted pregnancy to term.10
-
American Society for Reproductive Medicine (ASRM). “Fact Sheet: Dilation and Curettage.” 2014. <dilation_and_curettage_factsheet.pdf>.
-
Bloigu A, et al. “Immediate Complications after Medical Compared With Surgical Termination of Pregnancy.” Obstetrics & Gynecology, Vol 114, No. 4, October, 2009. <http://www.ncbi.nlm.nih.gov/pubmed/19888037>.
-
Alexander, Greg R. “Preterm Birth: Causes, Consequences, and Prevention.” Institute of Medicine (US) Committee on Understanding Premature Birth and Assuring Healthy Outcomes Outcomes; Behrman RE, Butler AS, editors. Washington (DC): National Academies Press, 2007. <http://www.ncbi.nlm.nih.gov/books/NBK11386/>.
-
ASRM. <https://www.asrm.org/FACTSHEET_Dilation_and_Curettage>.
-
Barnhart, Kurt and Loraine K. Endres. “Spontaneous Second Trimester Uterine Rupture After Second Trimester Abortion.” Vol. 96, Issue 2, Nov. 2000, pp. 806-808.
-
Alexander, Greg R. <http://www.ncbi.nlm.nih.gov/books/NBK11386/>.
-
Jiang, Xiaozhang, et al. “Does D&C Affect Future Pregnancy Outcomes.”The Ochsner Journal, 7(4), Winter, 2007, pp. 173–176. <http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3096409/>.
-
Fergusson, David M with Joseph M. Boden and L. John Harwood. “Does abortion reduce the mental health risks of unwanted or unintended pregnancy? A re-appraisal of the evidence.” Australian & New Zealand Journal of Psychiatry, Sept. 2013, Vol. 47, No. 9, pp. 819-827. <http://www.ncbi.nlm.nih.gov/pubmed/23553240>.
how developed is the child at this point in pregnancy?
During this stage of pregnancy, the preborn child is developing rapidly. At four to five weeks LMP — that is, four to five weeks since the first day of the mother’s last period, and just two to three weeks following fertilization (conception) — the baby’s organs start to develop, and the heart begins to beat. These developmental milestones often take place before the mother even knows she is pregnant.
Week 8
At eight weeks LMP, the preborn baby’s hands and feet are developing, and the neural pathways in her brain start to form. The child is constantly moving in the womb, although the mother cannot feel it. Source: Baby Center.

Week 9
By nine weeks LMP, the child can suck her thumb, open and close her jaw, stretch, and sigh. The baby’s teeth begin to form and the heart completes dividing into four chambers. Source: Baby Center.

Week 10
At week ten LMP, the child’s vital organs have developed and start to function. The baby is rapidly moving in the uterus, and tiny nails begin to form on the child’s hands and feet. Source: Baby Center.

Week 12
At twelve weeks LMP, the child develops reflexes, and can open and close fingers, respond to touch, and make movements with his or her mouth. The child’s nerve cells are developing rapidly. Source: Baby Center.

Please note: This website has been researched and reviewed by physicians for medical accuracy; however, it is not intended to constitute medical advice or replace the individualized counsel of a doctor.
ABORTION PILLS
First Trimester Medical Abortion
A medical (or chemical) abortion is a non-surgical form of abortion in which the woman takes pills containing Mifepristone (RU-486) and Misoprostol (or Cytotec) to end the life of the baby. This procedure is performed during the first trimester of pregnancy. The drugs are approved by the FDA for use up to ten weeks since the first day of her last menstrual period (LMP).
how is a medical abortion performed?
The woman visits an abortion clinic or doctor’s office and ingests pills containing Mifepristone (also known as RU-486) at the clinic. This drug blocks the action of the hormone called “progesterone,” which is naturally produced by the mother’s body to enable the mother to sustain and nourish the pregnancy. When RU-486 blocks progesterone, the lining of the mother’s uterus breaks down, cutting off blood and nourishment to the baby, who then dies inside the mother’s womb. Twenty-four to forty-eight hours later, the woman ingests another drug called Misoprostol (also called Cytotec), administered orally or vaginally, which causes contractions and bleeding to expel the baby from the womb.
what type of medical supervision occurs during a medical abortion?
The Food and Drug Administration (FDA) specified exactly how the drug regimen was to be given.
There is usually limited medical supervision for the woman during a medical/chemical abortion. Prior to the abortion, she should receive an exam that includes an ultrasound in order to confirm the pregnancy and diagnose any complicating factors, such as a tubal or ectopic pregnancy.
After taking the first pills (Mifepristone/RU-486) in the clinic, she is sent home to complete the abortion. This means she must correctly follow the directions for taking the remaining set of drugs and is responsible for judging whether her body’s reaction to the abortion is normal or not (such as a dangerous loss of blood). With this type of abortion, it is likely that she may not have a doctor to provide immediate help should a potentially life-threatening complication occur, so it is very important that she report any concerns to her doctor and seek emergency help if necessary.
The woman will also be responsible for disposing of her child’s remains. While she could lose her baby anytime and anywhere during this process, the woman will often sit on a toilet as she prepares to expel the remains, which she will usually then flush— she may even see her dead baby within the pregnancy sac.
It is also important that the abortionist perform a follow-up exam and ultrasound to ensure that the abortion is complete.
what if a mother changes her mind after taking the ru-486 abortion pill?
If a mother changes her mind after taking RU-486, she might still be able to save her baby, especially if she has not yet ingested the second drug, Misoprostol. To increase her chances of saving the baby, progesterone must be administered as soon as possible to counteract the effects of RU-486. Helpful guidance, resources, and stories of successful abortion pill reversals are available at abortionpillreversal.com.
Get Help
what are the short-term and long-term risks and adverse effects of medical abortion?
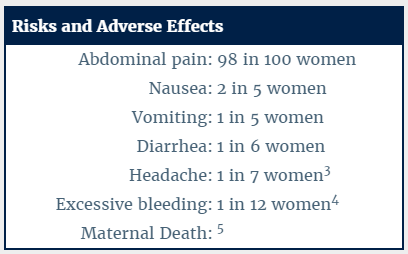
In the short term, RU-486 and Misoprostol cause severe cramping, contractions, and heavy bleeding, which force the dead baby out of the mother’s uterus. Contractions and bleeding to expel the baby can last from several hours to several days, and can be very intense and painful. Many women also experience nausea, vomiting, diarrhea, abdominal pain, and headache.1 Maternal deaths have occurred, most frequently due to infection and undiagnosed ectopic pregnancy.2
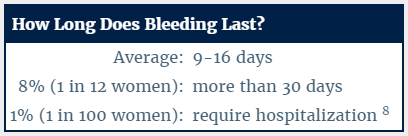
Even after the baby is expelled, the bleeding and spotting may continue for several weeks. Bleeding usually lasts 9 to 16 days. Eight percent of women (1 in 12) bleed more than 30 days, and 1 percent require hospitalization because of heavy bleeding.6
About 5-8 out of 100 women (5-8%) may need a surgical procedure to complete the abortion or to stop too much bleeding.7
There is insufficient reporting on the long-term effects of medical abortions. Approval for RU-486 in the United States only extends back to October, 2000, and long-term effects and risks must still be evaluated. This means women who undergo medical abortions could be prone to unknown risks.
There are studies that indicate the risk of depression, anxiety, and suicide is greater for a woman who aborts an unwanted pregnancy than it is for a woman who carries an unwanted pregnancy to term.9
-
Von Hertzen, H, et al. “Misoprostol Dose and Route after Mifepristone for Early Medical Abortion: A Randomised Controlled Noninferiority Trial.” British Journal of Obstetrics and Gynaecology, June 18, 2010. <onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2010.02636.x/full>.
-
Ellertson,Charlotte, et al. “Can women use medical abortion without medical supervision?” Reproductive Health Matters, Vol. 5, No. 9, Abortion: Unfinished Business, May 1997, pp. 149-161. <http://www.rhm-elsevier.com/article/S0968-8080(97)90019-7/abstract>.
-
Von Hertzen, H, et al. <onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2010.02636.x/full>.
-
Food and Drug Administration. “MIFEPREX (mifepristone) Tablets, 200 mg.” accessed 19 Jan. 2016. <http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020687s015lbl.pdf>.
-
Grimes, D.A. “Risks of mifepristone abortion in context.” Contraception, Vol. 71, 2005, p. 161. <https://www.arhp.org/uploadDocs/journaleditorialmar2005.pdf>.
-
Food and Drug Administration. “MIFEPREX (mifepristone) Tablets, 200 mg.”, <http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020687s015lbl.pdf>.
-
Food and Drug Administration. “MEDICATION GUIDE Mifeprex.” accessed 19 Jan. 2016 <http://www.fda.gov/downloads/Drugs/Drugsafety/ucm088643.pdf>.
-
Food and Drug Administration. “MIFEPREX (mifepristone) Tablets, 200 mg.”, <http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020687s015lbl.pdf>.
-
Fergusson, David M with Joseph M. Boden and L. John Harwood. “Does abortion reduce the mental health risks of unwanted or unintended pregnancy? A re-appraisal of the evidence.” Australian & New Zealand Journal of Psychiatry, Sept. 2013, Vol. 47, No. 9, pp. 819-827. <http://www.ncbi.nlm.nih.gov/pubmed/23553240>.
what are the failure rates for medical abortion?
The failure rates for medical abortion increase as the pregnancy progresses.
According to the FDA’s assessment, using published and unpublished studies, the failure rate of RU-486 rises to over 7.3% when administered in the 10th week. This is more than three times higher than their assessed failure rate for RU-486 abortions in the 7th week.
Other studies have recorded even higher failure rates for medical abortion. The Von Hertzen study found failure rates of 5% at seven weeks and under, 8% at eight weeks, and 10% at nine weeks.
-
Von Hertzen, H, et al. “Misoprostol Dose and Route after Mifepristone for Early Medical Abortion: A Randomised Controlled Noninferiority Trial.” British Journal of Obstetrics and Gynaecology, June 18, 2010. <onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2010.02636.x/full>.
-
Von Hertzen. <onlinelibrary.wiley.com/doi/10.1111/j.1471-0528.2010.02636.x/full>.
how developed is the child at this point in pregnancy?
During this stage of pregnancy, the preborn child is developing rapidly. At four to five weeks LMP — that is, four to five weeks since the first day of the mother’s last period, and just two to three weeks following fertilization (conception) — the baby’s organs start to develop, and the heart begins to beat. These developmental milestones often take place before the mother even knows she is pregnant.
Week 8
At eight weeks LMP, the preborn baby’s hands and feet are developing, and the neural pathways in her brain start to form. The child is constantly moving in the womb, although the mother cannot feel it. Source: Baby Center.
Week 9
By nine weeks LMP, the child can suck her thumb, open and close her jaw, stretch, and sigh. The baby’s teeth begin to form and the heart completes dividing into four chambers. Source: Baby Center.
Please note: This website has been researched and reviewed by physicians for medical accuracy; however, it is not intended to constitute medical advice or replace the individualized counsel of a doctor.
INDUCTION ABORTION
Third Trimester
A third trimester induction abortion is performed at 25 weeks LMP (25 weeks since the first day of the woman’s last period) to term. At 25 weeks, a baby is almost fully-developed and is considered viable, meaning he or she could survive outside the womb. For this reason, the abortionist will usually first kill the baby in utero by injecting a substance that causes cardiac arrest, and induces the mother’s labor to deliver her baby stillborn.
how is an induction abortion performed?
Day 1: To help ensure the baby will be delivered dead and not alive, the abortionist uses a large needle to inject digoxin or potassium chloride through the woman’s abdomen or vagina, targeting the baby’s heart, torso, or head. When the digoxin takes effect, the lethal dose causes a fatal cardiac arrest, and the baby’s life will end. (Even if the needle misses the baby, digoxin can still kill the baby when released into the amniotic sack, but will usually take longer to kill the child.)
During the same visit, the abortionist inserts multiple laminaria sticks, or sterilized seaweed, to open up the woman’s cervix.
Day 2: The abortionist replaces the laminaria and may perform a second ultrasound to ensure that the baby is dead. If the child is still alive, the abortionist administers a second lethal dose of digoxin or potassium chloride. During this visit, the abortionist may administer labor-inducing drugs.
The woman goes back to where she is staying while her cervix continues to dilate. The woman will usually wait a period of two to four days for her cervix to dilate enough for her to deliver the dead baby.
Day 3 or 4: The woman returns to the clinic to deliver her dead baby. If she goes into labor before she can make it to the abortion clinic in time, she will deliver her baby at home or in a hotel room. During this time, a woman may be advised to sit on a bathroom toilet until the abortionist arrives. If she can make it to the clinic, she will do so during her most heavy and severe contractions and deliver the dead baby.
If the child does not come out whole, the procedure becomes a D&E, or a dilation and evacuation. The abortionist uses clamps and forceps to dismember and remove the baby piece by piece.1
-
Darney, P.D., et al. “Digoxin to facilitate late second-trimester abortion: a randomized, masked, placebo-controlled trial.,” Obstetrics and Gynecology, Vol. 97, Issue 3, Mar.2001, pp. 471-476. <www.ncbi.nlm.nih.gov/pubmed/11239659>.
what if a woman changes her mind after laminaria insertion?
If a woman has been dilated with laminaria, but not yet undergone the surgical abortion, she can still change her mind. Depending on how much her cervix has dilated, there is a potential risk of miscarriage as dilation continues because her body may begin contractions and labor. A woman who changes her mind should immediately contact a medical professional to ensure the laminaria is properly removed.1
-
Kaufman, K. The Abortion Resource Handbook.” New York: Fireside, 1997, 32, 153. <https://books.google.com/books?id=F7q3TB6_koYC&pg=PR18&dq=the+abortion+resource+handbook&hl=en&sa=X&ved=0ahUKEwjBpZvBxNrJAhUO42MKHchnCA4Q6AEIJjAA#v=onepage&q=the%20abortion%20resource%20handbook&f=false>.
Get Help
what type of medical supervision occurs during an induction abortion?
After administration of the digoxin or potassium chloride, laminaria, and labor-inducing drugs, the woman often waits for labor at home or in a hotel. If she cannot make it to the abortion clinic in time for her delivery, she may be advised to call the abortion clinic and labor over the toilet. During this time, the woman does not have direct or immediate supervision.
what are the short-term and long-term risks and adverse effects of induction abortion?
A woman faces greater risks aborting her child in the late-term, given the child’s size and development. Late-term abortions have a high risk of hemorrhage, lacerations, and uterine perforations, as well as a risk of maternal death. Future pregnancies are also at a greater risk for loss or premature delivery due to abortion-related trauma and injury to the cervix.
There are studies that indicate the risk of depression, anxiety, and suicide is greater for a woman who aborts an unwanted pregnancy than it is for a woman who carries an unwanted pregnancy to term.1
-
Fergusson, David M with Joseph M. Boden and L. John Harwood. “Does abortion reduce the mental health risks of unwanted or unintended pregnancy? A re-appraisal of the evidence.” Australian & New Zealand Journal of Psychiatry, Sept. 2013, Vol. 47, No. 9, pp. 819-827. <http://www.ncbi.nlm.nih.gov/pubmed/23553240>.
are late-term abortions legal in the united states?
While some states have enacted prohibitions on abortion — including restricting the procedure after a certain point in pregnancy — other states permit abortions without exception.
how developed is the child at this point in pregnancy?
At 25 weeks, a preborn child is fully developed and considered viable — that is, with proper medical care and attention, he or she would be able to survive outside of the womb. While medical staff is required to provide life-saving care to a child who survives an abortion procedure, it is unlikely that doctors and hospitals will take intensive measures to rescue the baby if it is born alive following an abortion procedure.1
Week 25
At twenty-five weeks LMP, the baby’s hair continues to grow, and the color and texture can be discerned. At this stage, the child is around 13 ½ inches long, from the baby’s head to its heels. Source: Baby Center.

Week 27
At twenty-seven weeks LMP, the preborn baby weighs almost two pounds. The child’s brain tissue continues to develop, and the baby is sleeping and waking in regular cycles. The mother may even feel the child hiccup at this stage, which may become more common as the pregnancy progresses. Source: Baby Center.

Week 31
At thirty-one weeks LMP, the baby can turn his or her head to the side, and is very active in the womb. The baby kicks and does somersaults, and develops more fat underneath the skin. Source: Baby Center.
-
Grimes, David A. “Second-Trimester Abortions in the United States”, Family Planning Perspectives, Nov./Dec. 1984, 260-266.

Please note: This website has been researched and reviewed by physicians for medical accuracy; however, it is not intended to constitute medical advice or replace the individualized counsel of a doctor.
are you pregnant?
OPTION LINE
http://optionline.org | (800) 712-4357
Option Line offers a confidential live chat, text line, and toll-free phone line that is available 24/7. The website contains additional resources for women who are considering abortion, have had an abortion, or are seeking alternatives to abortion.
CARE NET
http://www.care-net.org/find-a-pregnancy-center | (866) 993-0794
Care Net offers free resources and a confidential, toll-free, phone line available from 10 AM to 6 PM EST.
have you had an abortion?
OPTION LINE
http://optionline.org | (800) 712-4357
Option Line offers a confidential live chat, text line, and toll-free phone line that is available 24/7. The website contains additional resources for women who are considering abortion, have had an abortion, or are seeking alternatives to abortion.
INTERNATIONAL HELPLINE FOR ABORTION RECOVERY
http://nationalhelpline.org | (866) 482-5433
International Helpline for Abortion Recovery provides confidential care 24/7 for those needing help after abortion. The helpline is staffed by consultants who have personally experienced the pain of abortion, but have also found hope and healing.
RACHEL’S VINEYARD
www.rachelsvineyard.org | (877) 467-3463 | rachel@rachelsvineyard.org
Rachel’s Vineyard offers confidential, weekend programs and other services across the United States and Canada, with additional sites around the world, for anyone affected by abortion.
are you an abortion worker?
AND THEN THERE WERE NONE
http://abortionworker.com/ | (888) 570-5501
And Then There Were None offers abortion workers a way out of the abortion industry by offering job recruitment services, legal help, emotional support, financial assistance, and professional counseling. They also hold all expense paid retreats for those who are interested in more intensive healing. All services are completely confidential.
have you taken the abortion pill?
ABORTION PILL REVERSAL
abortionpillreversal.com | (877) 558-0333
Abortion Pill Reversal offers a 24/7 hotline, staffed by medical professionals, for women seeking an abortion pill reversal. The APR program has a network of over 270 physicians worldwide to assist people who call the hotline.
are you interested in adoption?
BETHANY CHRISTIAN SERVICES
https://impregnant.org/adoption | (844) 838-4269
Bethany Christian Services is an international social service agency based in Grand Rapids, Michigan, that cares deeply about expectant parents, families and children. They provide free, confidential support for women and men facing unplanned pregnancy, with services including adoption, foster care, and pregnancy counseling available across the United States and around the world. Their toll-free phone line is operated 24/7.
AMERICAN ADOPTIONS
http://www.americanadoptions.com | (800) 236-7846
American Adoptions is a fully licensed, not-for-profit domestic adoption agency that works across the nation, and is currently one of the largest domestic adoption agencies of its kind in the United States. Adoption professionals are available 24/7 at the toll-free phone line.
SAFE HAVEN ALLIANCE
http://www.nationalsafehavenalliance.org/ | (888) 510-2229
The National Safe Haven Alliance (NSHA) is dedicated to reaching these women and encouraging them to make the right choice for themselves and their babies, whether it is a safe-haven relinquishment, adoption, or parenting. The toll-free crisis hotline is staffed 24/7.
Please note: This website has been researched and reviewed by physicians for medical accuracy; however, it is not intended to constitute medical advice or replace the individualized counsel of a doctor.
Featured

